
 MENU
MENU
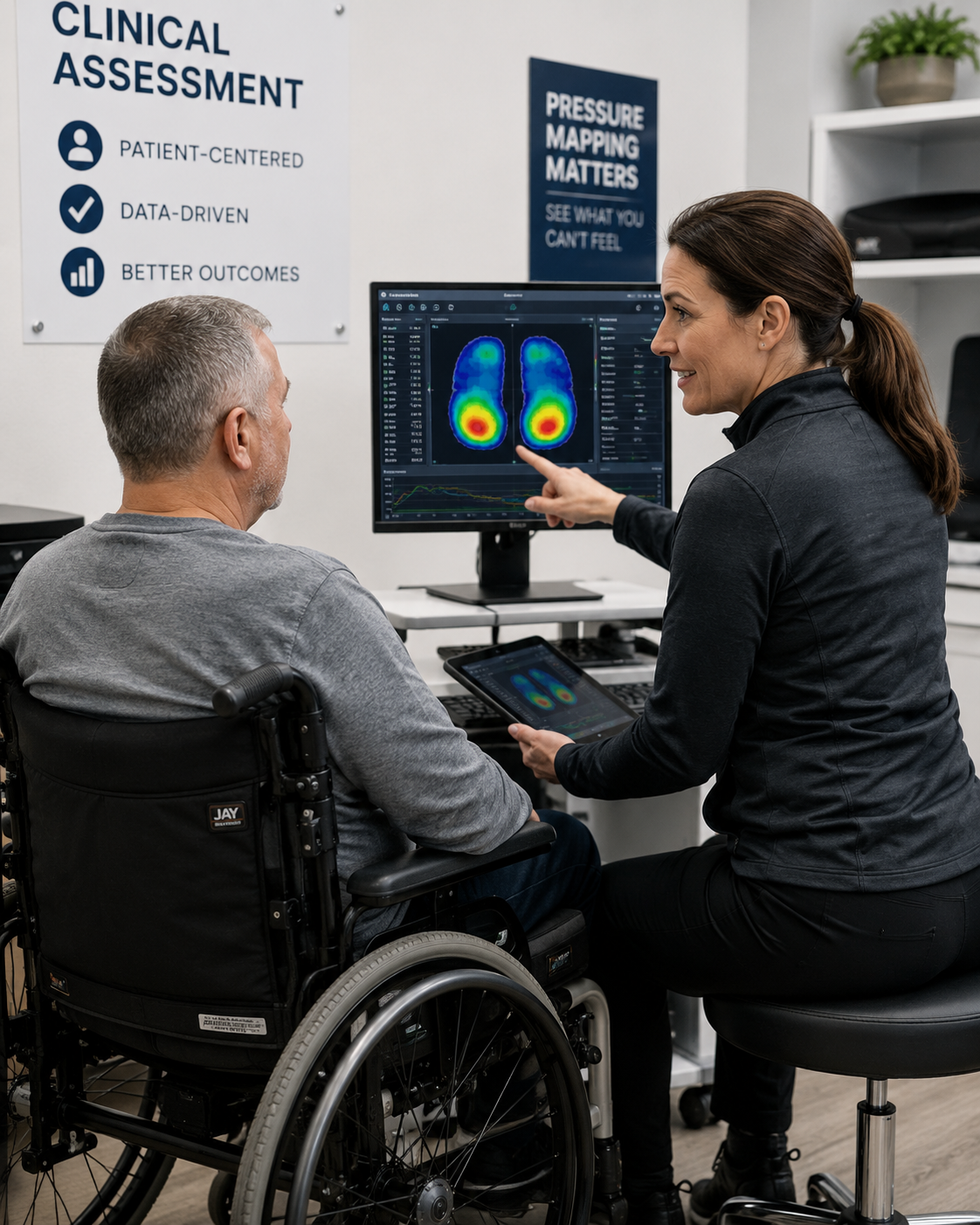
Pressure Mapping for Pressure Injury Prevention
CLINICAL PRESSURE ASSESSMENT PROGRAM
Objective interface pressure data for mattress and wheelchair seating assessment.
Blue Chip Medical supplies clinical pressure mapping systems for both mattress and wheelchair seating assessment to hospitals, VA hospitals, rehabilitation facilities, skilled nursing facilities, and wound care programs across the United States. Both systems use Tactilus piezoresistive sensor technology and are manufactured in the USA.


Tactilus Pressure Mapping Systems — Mattress and Seating | Blue Chip Medical
Pressure mapping is the objective measurement of interface pressure — the force per unit area between a patient’s body and a support surface. Clinicians use pressure mapping to identify anatomical zones where sustained pressure exceeds capillary closing threshold, quantify the pressure redistribution performance of specific therapeutic surfaces for individual patients, and generate documented clinical evidence for surface selection, repositioning protocols, and payor justification.
Why Pressure Mapping Belongs in Every Pressure Injury Prevention Program
OBJECTIVE DATA. BETTER OUTCOMES.
Pressure injury prevention programs have historically relied on risk stratification tools, repositioning schedules, and clinical observation. These methods identify patients at risk. They do not measure the actual mechanical forces acting on that patient’s tissue at any given moment on any given surface.
Interface pressure — the measurable force between a patient’s body and the surface supporting it — is the primary mechanical variable in pressure injury development. A patient scored as high-risk on the Braden Scale may generate acceptable interface pressure on a well-fitted therapeutic surface. A patient scored as moderate-risk may generate dangerously elevated pressure on an inadequate surface. The Braden Scale cannot tell the difference. Pressure mapping can.
Pressure mapping shifts clinical decision-making from probability to measurement. It gives wound care nurses, seating specialists, physical therapists, and facility administrators a direct, reproducible data point — the actual interface pressure this patient generates on this surface — that risk scores cannot provide. That data informs surface selection, repositioning interval adjustment, cushion configuration, and the clinical documentation that supports payor authorization and regulatory compliance.
Blue Chip Medical Pressure Mapping Systems
MATTRESS AND SEATING ASSESSMENT
Blue Chip Medical supplies two Tactilus-based pressure mapping systems designed for the distinct clinical demands of mattress and wheelchair seating assessment. Both operate on the same piezoresistive sensor platform and share a unified Windows-based clinical interface.

Mattress Pressure Mapping System: Tactilus
The Tactilus mattress system maps interface pressure across the full body contact area in supine positioning. 1,612 discrete sensing points cover a 32″ x 80″ sensing area, capturing peak pressure at the sacrum, heels, trochanters, scapulae, and occiput in real time. Supplied to hospitals, VA hospitals, long-term care facilities, and wound care clinics. Model TACT-Y-TS10. Manufactured in the USA.

Wheelchair Pressure Mapping System: Tactilus
The Tactilus seating system maps interface pressure in seated positioning across a 20″ x 20″ sensing area with 1,024 discrete sensing points. Quadrant monitoring identifies asymmetric ischial loading. Side-by-side comparison of up to three cushions simultaneously supports Medicare and Medicaid DME documentation. Supplied to hospitals, VA hospitals, rehabilitation facilities, and seating clinics. Manufactured in the USA.
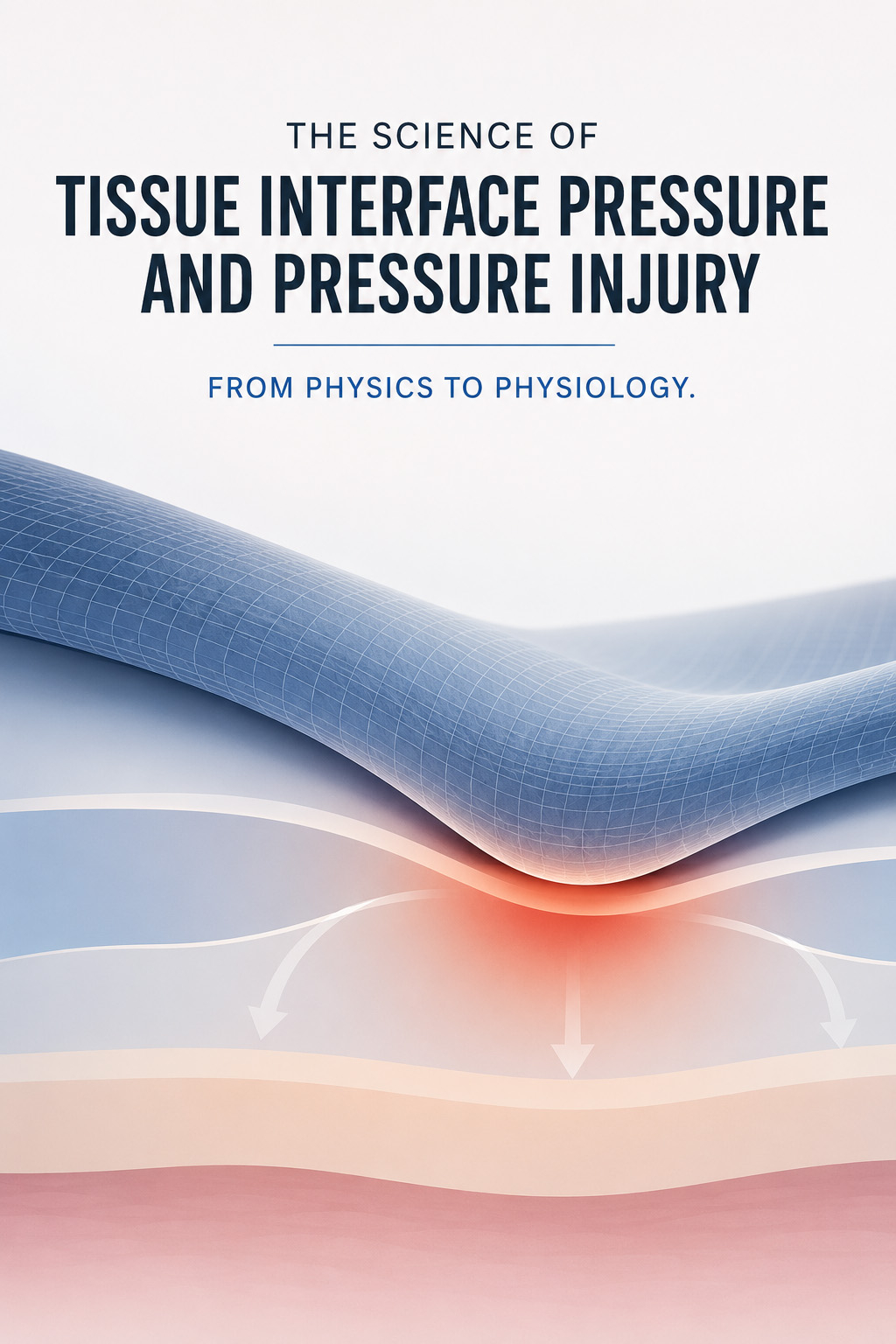
The Science of Tissue Interface Pressure and Pressure Injury
FROM PHYSICS TO PHYSIOLOGY
Pressure injuries are a mechanical phenomenon. Soft tissue compressed between a bony prominence and an external surface sustains a reduction in microcirculatory blood flow proportional to the magnitude and duration of the applied pressure. When interface pressure exceeds capillary closing pressure — typically cited at 32 mmHg — perfusion to the overlying soft tissue is restricted. If sustained, ischemic injury begins.
The relationship between pressure, time, and tissue damage is not linear. Low pressures sustained for extended periods cause cumulative damage equivalent to, or greater than, brief exposure to high pressures. This pressure-time relationship is clinically significant in every setting where patients remain on the same surface for hours: ICU patients who cannot reposition, wheelchair users who sit for a full day without weight-shifting, and long-term care residents whose surfaces are rarely evaluated after initial placement.
Tissue damage does not always announce itself at the surface. Deep tissue pressure injury (DTPI) begins at the level of bone and muscle, where interface pressure concentrates. By the time discoloration or surface breakdown appears, significant subsurface damage may already have occurred. This is the clinical case for early, objective measurement. Waiting for visible signs is waiting for injury that has already happened.
Three factors compound the mechanical pressure effect:
- Shear force: Tangential forces at the skin-surface interface during movement, head-of-bed elevation, and transfers damage microvascular structures independent of direct compression
- Microclimate: Elevated skin temperature and moisture reduce tissue tolerance to pressure, lowering the threshold at which ischemic injury initiates
- Tissue tolerance: Neurological impairment, malnutrition, vascular disease, and advanced age all reduce the tissue’s capacity to withstand and recover from pressure loading
Patient Populations That Benefit Most From Pressure Mapping
HIGH RISK. MEASURABLE. PREVENTABLE.
Pressure mapping adds the most clinical value where standard risk assessment is insufficient, repositioning is limited or impossible, and the consequences of inadequate surface selection are most severe.
Spinal Cord Injury
SCI patients are the highest-risk population for both mattress and seating pressure injuries. Absent sensation eliminates the feedback mechanism that alerts intact patients to shift position. Altered autonomic regulation impairs tissue perfusion. Muscle atrophy reduces soft tissue cushioning over bony prominences. SCI patients require pressure mapping for both mattress assessment during inpatient care and wheelchair seating assessment throughout their lifetime.
ICU and Critical Care
Sedated, paralyzed, and post-surgical ICU patients cannot self-reposition and cannot communicate discomfort. Standard two-hour turning schedules are not individualized to the actual interface pressure each patient generates on their current surface. Pressure mapping provides objective data to determine whether a patient’s surface is adequate and whether repositioning intervals should be adjusted based on measured pressure rather than protocol defaults.
Neurological Conditions
Stroke, TBI, and multiple sclerosis patients share the SCI risk profile to varying degrees — reduced or absent sensation, impaired motor function, and limited self-repositioning capacity. Stroke patients with hemiplegia generate asymmetric pressure distribution in both supine and seated positioning. TBI patients in acute care may be unresponsive for extended periods requiring objective pressure assessment.
Bariatric Patients
Bariatric patients generate pressure distribution patterns that differ substantially from standard-weight populations. Standard interface pressure norms and surface recommendations may not apply. Body weight concentrates over a different geometric distribution, and available therapeutic surfaces vary significantly in their capacity to immerse and envelop high-BMI patients. Pressure mapping provides direct measurement of the actual pressure this patient generates on this surface.
Geriatric and Long-Term Care Residents
Aging reduces tissue tolerance through decreased subcutaneous tissue, impaired microvascular response, and malnutrition risk. Geriatric patients in long-term care may remain on the same mattress and wheelchair cushion for years without objective reassessment. Pressure mapping identifies residents whose surfaces have become clinically insufficient and provides documented evidence for therapeutic upgrade justification.
Post-Surgical and Immobile Inpatients
Post-surgical patients are immobile for defined recovery periods. Operative positioning itself generates sustained interface pressure at the sacrum and heels that may produce injuries apparent in the days following procedures. Pressure mapping supports surface selection for post-operative recovery positioning and early identification of at-risk zones before breakdown occurs.
Pressure Mapping and the NPIAP Clinical Framework
ALIGNED WITH EVIDENCE-BASED STANDARDS
The National Pressure Injury Advisory Panel (NPIAP) is the authoritative clinical and research organization for pressure injury prevention and management in the United States. NPIAP’s staging system — Stage I through Stage IV, plus unstageable and deep tissue pressure injury — provides the classification framework used across acute care, long-term care, and rehabilitation settings.
NPIAP clinical practice recommendations include individualized surface selection as a core element of pressure injury prevention programs. Pressure mapping generates the patient-specific interface pressure data that makes individualized surface selection objective and documentable rather than observational and assumed. Pressure mapping supports NPIAP-aligned clinical practice at three levels:
- Prevention: Identifying patients whose current surface generates interface pressures above safe clinical thresholds before tissue injury occurs — enabling proactive surface selection rather than reactive wound management
- Assessment: Providing objective data on the mechanical environment contributing to an existing pressure injury, including whether the current surface is sustaining wound chronicity
- Outcomes: Generating reproducible, longitudinal pressure data that supports quality improvement initiatives, QAPI programs in SNF settings, and the clinical evidence base for prevention program effectiveness
The Braden Scale and Norton Scale remain validated risk stratification tools. Pressure mapping does not replace them. It provides a complementary, objective measurement those tools cannot generate — the actual interface pressure this patient is experiencing at this moment on this surface.

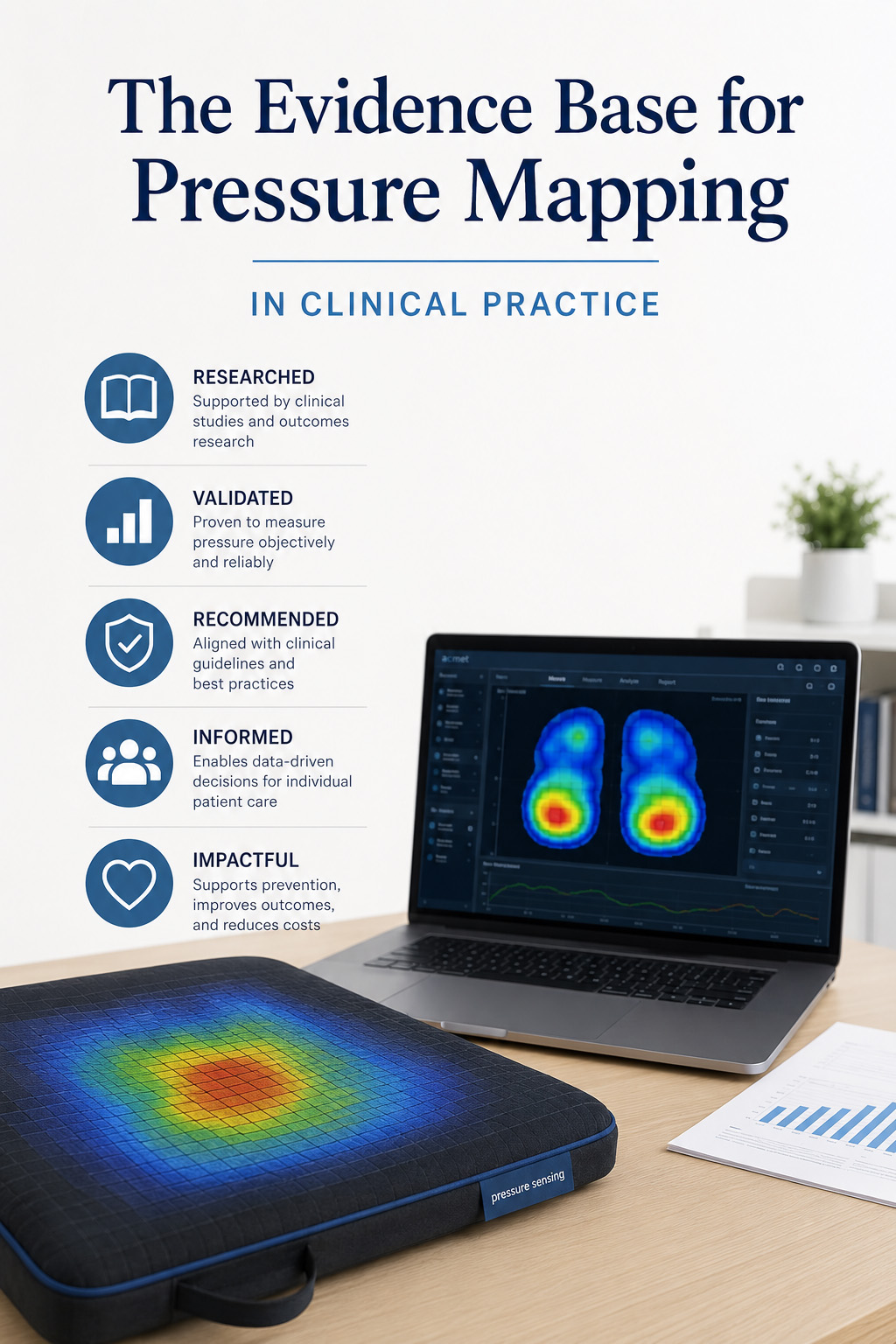
The Evidence Base for Pressure Mapping in Clinical Practice
RESEARCH-SUPPORTED. CLINICALLY VALIDATED.
The clinical evidence for pressure mapping in pressure injury prevention has grown substantially over the past two decades. The most clinically significant research area is continuous bedside pressure mapping (CBPM), which monitors interface pressure in real time throughout a patient’s care period rather than at discrete assessment points.
Peer-reviewed research on CBPM technology in ICU settings has documented up to 88% overall reduction in pressure injury risk compared to standard care. The mechanism is direct: real-time pressure visualization enables nursing staff to verify that repositioning has achieved adequate pressure offloading, rather than assuming a position change resolved elevated pressure at the high-risk zone.
Episodic pressure mapping — the modality used in Blue Chip Medical’s Tactilus systems — serves a distinct but complementary clinical function. Episodic mapping generates surface-specific, patient-specific interface pressure data at defined assessment points. This data:
- Quantifies the pressure redistribution performance of specific surfaces for individual patients
- Enables objective side-by-side comparison of up to three surfaces or cushions simultaneously
- Provides reproducible baseline measurements for longitudinal clinical monitoring
- Generates documented clinical evidence for surface selection decisions and payor justification
The clinical value of episodic mapping is in the quality of the decision it informs. A clinician who has mapped a patient on their current surface, compared results against two therapeutic alternatives, and selected the surface producing the most clinically appropriate pressure distribution has made a better-supported decision than one relying on observation alone. The documentation of that decision is an equally important clinical and operational output.
Building a Pressure Mapping Program: An Institutional Framework
FROM SINGLE TOOL TO CLINICAL PROGRAM
A single pressure mapping assessment is a data point. A pressure mapping program is a clinical infrastructure. Facilities that achieve measurable reduction in pressure injury incidence through pressure mapping share several structural characteristics.
Defined Assessment Triggers
Clear protocols for when pressure mapping is performed — on admission for high-risk patients, at surface change, when an existing pressure injury is not progressing, and on annual review for long-term residents and wheelchair users — ensure mapping data is collected at the moments when it can most influence clinical decisions.
Trained, Consistent Operators
Pressure mapping data is only as useful as the clinician interpreting it. Facilities with effective programs invest in training wound care nurses, seating specialists, and rehabilitation staff to read peak pressure outputs, interpret quadrant data, and translate mapping findings into specific surface and positioning recommendations.
Integrated Documentation
Mapping findings documented in the clinical record — not stored separately — become part of the wound care program record, support MDT communication, and generate the evidence trail facilities need for CMS compliance and survey readiness.
Bidirectional Assessment
Patients with both mattress and seating pressure exposure require assessment in both environments. A facility that maps mattress surfaces but not wheelchair cushions has an incomplete picture of total interface pressure exposure for its wheelchair-dependent population. Blue Chip Medical’s mattress and seating systems operate within the same clinical interface, enabling a unified assessment program across both environments.
Regular Reassessment
Patient condition, body composition, and mobility status change over time. A surface that was clinically appropriate at admission may be insufficient months later. Scheduled reassessment intervals — particularly for long-term care residents and SCI patients — ensure that mapping data remains current and actionable. Annual seating reassessment using pressure mapping is standard practice in SCI rehabilitation programs.
Blue Chip Medical: 30 Years of Support Surface Innovation
CLINICAL MANUFACTURER. OPERATIONAL EXPERTISE.
Blue Chip Medical Products has designed and manufactured therapeutic support surfaces and clinical pressure assessment tools for more than 30 years from its facility in Suffern, New York. The company’s product line spans alternating pressure mattresses, lateral rotation mattresses, advanced foam support surfaces, and the Tactilus pressure mapping program.
Blue Chip Medical’s pressure mapping program reflects the same operational orientation that defines the company’s support surface manufacturing. Products are designed for clinical deployment across diverse patient populations, built for durability in multi-patient institutional use, and specified with the precision that clinical documentation and payor authorization require.
Both Tactilus pressure mapping systems — mattress and wheelchair seating — are manufactured in the United States and supported by a clinical team with deep working knowledge of support surfaces, wound care, and patient handling across acute care, rehabilitation, and long-term care environments.
- 30+ years of therapeutic support surface manufacturing
- Alternating pressure mattresses and lateral rotation systems
- Advanced foam technologies for pressure redistribution
- Tactilus mattress and seating pressure mapping systems
- All products manufactured in the USA
Who Blue Chip Medical Supplies
INSTITUTIONAL SUPPLY. NATIONWIDE.
Blue Chip Medical supplies the Tactilus pressure mapping program to:
- Acute care hospitals and health systems
- VA hospitals and federal healthcare facilities
- Inpatient and outpatient rehabilitation centers
- Long-term care and skilled nursing facilities
- Seating clinics and assistive technology programs
- Home health agencies and DME providers
- Wound care programs and clinics
- Teaching hospitals and clinical research institutions
For institutional pricing, volume procurement, and clinical program support, contact Blue Chip Medical directly.
Call: 800-795-6115
Frequently Asked Questions: Pressure Mapping for Pressure Injury Prevention
What is pressure mapping in clinical care?
Pressure mapping is the objective measurement of interface pressure — the force per unit area between a patient’s body and a support surface — at the full contact area. Clinicians use pressure mapping data to identify high-risk zones, evaluate surface performance, optimize repositioning protocols, and generate documented clinical evidence for surface selection and payor authorization.
How does pressure mapping prevent pressure injuries?
Pressure mapping identifies the actual interface pressure a specific patient generates on a specific surface, enabling clinicians to determine whether that surface provides adequate pressure redistribution. It supports early surface changes before injury develops, individualized repositioning intervals based on measured pressure rather than protocol defaults, and objective documentation of prevention measures for wound care programs and regulatory compliance.
What is the difference between mattress and wheelchair seating pressure mapping?
Mattress pressure mapping assesses interface pressure in supine positioning across the full body contact area, capturing pressure at the sacrum, heels, trochanters, scapulae, and occiput. Wheelchair seating pressure mapping assesses interface pressure in seated positioning, focusing on the ischial tuberosities, sacrum, and coccyx with quadrant monitoring for asymmetric loading. Patients who use wheelchairs as their primary mobility device require assessment in both environments.
What evidence supports the use of pressure mapping in clinical practice?
Peer-reviewed research on continuous bedside pressure mapping technology in ICU settings has documented up to 88% overall reduction in pressure injury risk compared to standard care. Episodic pressure mapping generates the patient-specific, surface-specific data that informs the surface selection and repositioning decisions underlying those outcomes. Both modalities produce clinically actionable interface pressure data; the appropriate use depends on care setting and clinical goals.
What is interface pressure and why does it cause pressure injuries?
Interface pressure is the mechanical force applied per unit area at the contact point between a patient’s body and a support surface. Sustained interface pressure above approximately 32 mmHg — the capillary closing pressure threshold — restricts blood flow to overlying soft tissue, causing ischemia. If sustained, ischemia progresses to tissue deformation, cell death, and pressure injury. The damage process begins at the bone-tissue interface and may progress to the skin surface, which is why deep tissue pressure injury often precedes visible surface changes.
Who should perform pressure mapping assessments?
Mattress pressure mapping is most commonly performed by wound care nurses (including CWOCNs), physical therapists, and occupational therapists. Wheelchair seating pressure mapping is most commonly performed by Assistive Technology Professionals (ATPs), Certified Rehabilitation Technology Suppliers (CRTs), physical therapists, and occupational therapists. Both roles include clinical educators and research staff in teaching hospital settings.
How does pressure mapping support CMS compliance and regulatory documentation?
Pressure mapping data provides objective clinical evidence of proactive pressure injury prevention measures. In acute care, this supports Hospital-Acquired Condition (HAC) documentation. In skilled nursing facilities, mapping data supports QAPI program documentation and survey readiness. For DME authorization, mapping data provides the objective clinical evidence payors require to authorize therapeutic surfaces and wheelchair cushions.
Does Blue Chip Medical supply pressure mapping systems to VA hospitals?
Yes. Blue Chip Medical supplies both the Tactilus mattress pressure mapping system and the Tactilus wheelchair seating pressure mapping system to VA hospitals and federal healthcare facilities. VA patient populations — with high rates of spinal cord injury, neurological conditions, and complex comorbidities — represent an elevated-risk group for whom comprehensive pressure mapping programs covering both mattress and seating environments are clinically indicated.